What Does "Low-Resource Environment" Actually Mean?
Co-written with Summer Institute Manager Maddy Bishop-Van Horn.
At Engineering World Health, and more generally in the international development field, we often use the term “low-resource” — but what does this term mean for biomedical technicians and engineers?
In high-income countries, when equipment breaks down, either a new component is ordered from the manufacturer or the entire machine is replaced.
Often, neither of these options is available in low-resource settings. The vast majority of medical equipment is manufactured in high-income countries such as the United States, Germany, and Japan. Much of the equipment found in low-income country hospitals is donated, without access to customer service, user training, or sometimes even instruction manuals. While more generic spare parts may be easy to find in the countries where we work, specialized parts such as equipment-specific light bulbs and printed circuit boards are challenging if not impossible to find and replace. Even if the part itself is very inexpensive, if it can’t be found in-country, it can cost hundreds of dollars and take several months to ship to the hospital. Parts must be ordered from the manufacturer or specific dealers. There is no 2-hour Amazon Prime shipping in Kigali, Rwanda… yet.
Hospital technicians do not always have the time or budget to go looking for spare parts. It’s not uncommon for the technicians to also be responsible for keeping the ambulance running and the lights on at the hospital. When hospital technicians do not have access to necessary spare parts, the equipment falls out of service, and doctors are unable to properly diagnose and treat patients.
While EWH cannot make specialized parts available, our Institute participants do have time to look for supplies, and have a small discretionary budget to spend on spare parts that have the potential to immediately put important equipment back into service. Although medical equipment manufacturers may be far away, EWH participants find other resources that help hospital staff find innovative and more locally sustainable solutions for their hospitals.
So what resources are available?
- Parts from cars, motorcycles, and household appliances: In general, the first instinct in low-resource settings is to repair instead of replace. Markets for spare automotive and appliance parts are common because there are more cars and appliances than there are medical devices. Parts for cars, especially the older cars found in low-resource environments, tend to be more standardized than parts for medical equipment. The people running the markets have lots of experience making repairs.
The UNSW design team created an uninterruptible surgical light using car headlights and batteries, so that the lights stay on even if power goes out during surgery. Car headlights are much cheaper and easier to find than specialized lights for surgical lamps.
One source of spare parts for medical devices is other medical devices. Technicians and EWH participants are often able to find several of the same kind of equipment in storage rooms or equipment graveyards. From five broken centrifuges, they may be able to find enough spare parts to reassemble three working centrifuges.
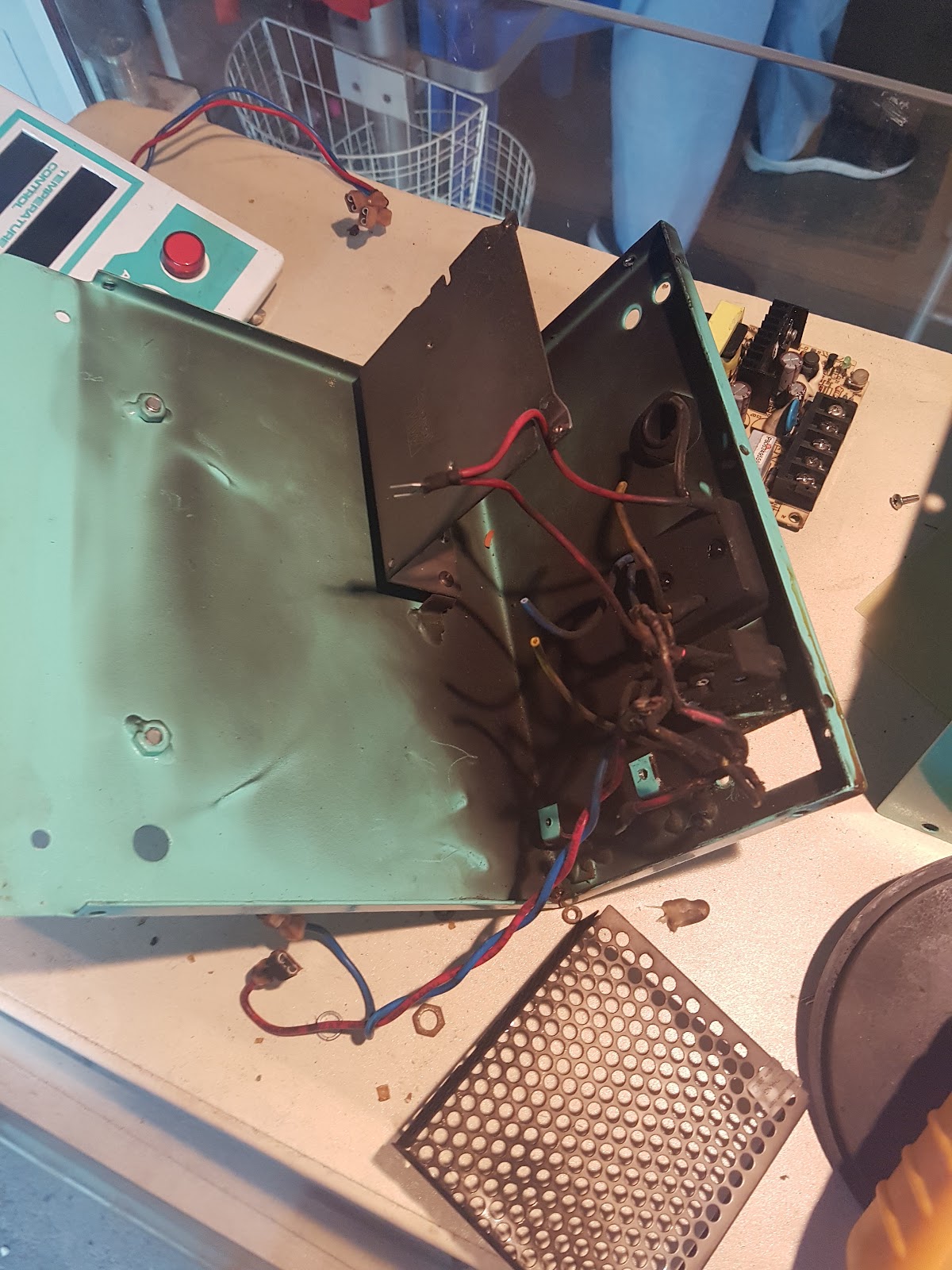
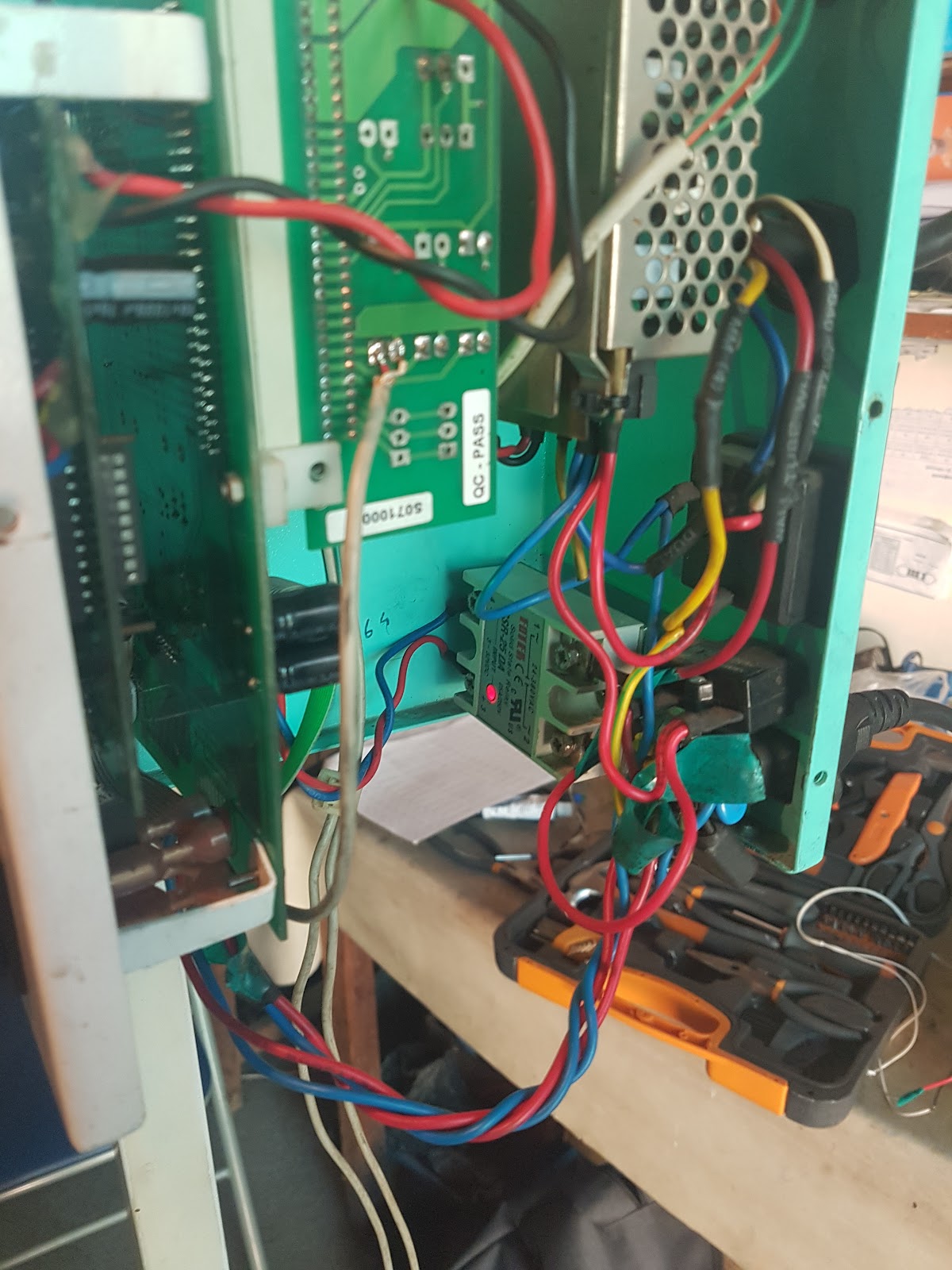
One team in the January Institute in Cambodia in 2018 found two out-of-service infant warmers. The inside of one was completely burnt out. The team’s final fix was to swap a few circuit boards between the two infant warmer and replace a relay. They were able to return the repaired infant warmer to NICU.

During the Summer Institute in Nicaragua in 2017, a group of participants found two centrifuges in the hospital’s equipment graveyard. With parts from one broken machine, the group was able to repair one of the centrifugues and return it to the hospital’s lab.
- Welding: Even some of the smallest, most rural towns we work in have a welder! Welders typically repair cars, motorcycles, build railings, and other metalwork. EWH participants often contract their services for projects to benefit the hospital.
EWH participants often find that oxygen canisters are not being carried safely. One group consulted with local staff, designed a safer solution, and hired a local welder to make it happen.
EWH participants in Cambodia found a broken gurney that required welding. They rode their bicycles around town, found a man with a welding machine, and were able to communicate their need. The welder and his friend drove to the hospital, picked up the broken gurney, brought it home and repaired it, and then returned it to the hospital.
- Carpentry: Furniture in low-resource settings is often built locally because it is cheaper than importing furniture. For this reason, many towns have skilled carpenters. Much like the welders, EWH participants have been able to hire carpenters for special projects.
Many hospitals lack seating options, both in waiting rooms and in wards. After speaking with a nurse in the pediatric department, EWH participants in Rwanda hired a local carpenter to build stools and benches for parents of patients to sit on.
- Electronics and hardware shops: Sometimes found in the same markets that sell meat and produce, electronics and hardware shops are usually family-owned and packed with tools and components, new and used. These small shops are the first place technicians and EWH participants alike look for spare parts.
EWH participants are often surprised at what they can find at shops such as the ones above. Shopping for spare parts and tools is one rewarding way participants immerse in local life.
- Human resources: Humans are adaptive and resilient. People in low-resource environments are incredibly accomplished at innovating new solutions with the resources available. A nurse trained to use a new infant incubator can train the rest of the maternity ward. Technicians with limited formal training but years of experience may quickly diagnose a broken centrifuge or build a specialized tool in order to open up a machine for service. Regardless of where you are in the world, people are at the center of healthcare, and it’s people who make healthcare work.





These resources aren’t a replacement for the equipment and parts manufacturers available in high-income countries. However, when they’re all brought together, remarkable solutions can be found that put equipment back to work diagnosing and treating patients.
At the end of the day, all resources on this planet are finite. EWH participants find themselves better problem solvers from exposure both to low-resource environments and the dedicated staff who make our partner hospitals run despite the challenges.